- 400-500 BC: Humorism
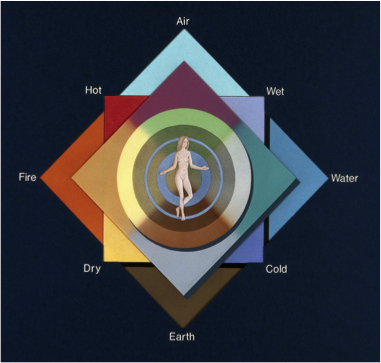
Figure 1: Humorism
Humorism was an early theory for the mechanisms of the body. Hippocrates (400-500BC) stated that illness was caused by an imbalance of four humours; blood, phlegm, yellow bile, and black bile (Stelmack and Stalikas 1991, 257), an idea that reigned until the 17th Century (Bos 2009, 29). Galen (Hague 1991) later linked blood to a sanguine disposition (hopeful); yellow bile to a choleric one (easily angered), phlegm to a phlegmatic one (calm, neutral); and black bile to melancholia (sadness). It was understood that imbalances could be adjusted with physical treatments, such as bloodletting and emetics that would remove a humour that was in excess (Androutsos et al 2008, 32), and bleeding and vomiting were evidence that the imbalance was rectified.
Humorism provided a holistic view of wellness that acknowledged the importance of both physical and environmental factors, such as diet and exercise (Telles-Correia and Marques 2015). It was predominately a departure from supernatural ideology and the role of the gods, in favour of the concept that physical and mental health were intrinsically linked (Bos 2009, 31). Bos (2009, 29) believes the decline is linked to a parting from a focus on character in favour of alternative theories. Nevertheless, the idea of balance remains prevalent.
2. From the 17th C: The Asylum

Figure 2: Bethlehem Hospital 1714
The concept of locking up the insane began in the late 17th Century (Porter 2002, 51-52). The Asylum was an institution based on moral therapy; the premise that psychology and compassion could be used to treat severe mental illness (Rosenblatt 1984). Prior to this, individuals were largely kept in the community (Porter 2002). One of the earliest hospitals was Tuke’s York Retreat (1796) (Rosenblatt 1984, 246), which echoed the theory of Pinel breaking patient chains (Porter 2002, 58). Both advocated for routines, pleasant surrounds and to abolish restraint.
The asylums were self-contained yet isolated, with architecture that was part of the treatment (Porter 2002, 62). Early on, conditions varied greatly and following outrage at abuse of patients like William Norris at the Bethlehem Hospital (1814), a move was made towards regulation through the Mad House Act of 1828 (Wiles 2016). However, due to overpopulation, patient care declined and by the 1890s more were leaving dead than cured, influencing consequent deinstitutionalisation (Wiles 2016, Porter 2002, 64).
Originating as a place of refuge, asylums were a sign and place of progress (Porter 2002, 65). While it is argued that moving the focus from the body to the mind merely meant switching repression type (Foucault, 1988, 266), this does not warrant overlooking the introduction of compassion, hope and a person-central approach (Shorter, 1997, 4).
3. 1939: Electro-Convulsive Therapy
 Figure 3: Australian ECT Machine (Melbourne Museum 2017)
Figure 3: Australian ECT Machine (Melbourne Museum 2017)
Electro-convulsive therapy (ECT) is arguably the greatest discovery of psychiatry, and the most effective and empirical treatment (Shorter and Healy 2007, 2).
Replacing chemical alternatives such as metrazol and insulin, both dangerous and less successful, it is a form of shock therapy (1935; Shorter and Healy 2007, 6) which was based on Meduna’s idea that schizophrenia was an antagonist of epilepsy. The concept was to treat symptoms by disrupting brain activity through seizures, coma or loss of consciousness (Piotrowski and Guerra 2016). The development of the Bini-Cerletti ECT machine was motivated by the desire to find a safer treatment.
4. 1951: The First Antipsychotic (Chlorpromazine)
Laborit’s and Rhone-Poulence’s discovery of Chlorpromazine (1951), the first antipsychotic, was a precursor to the rapid development of the psychopharmacology industry (Ban 2007).
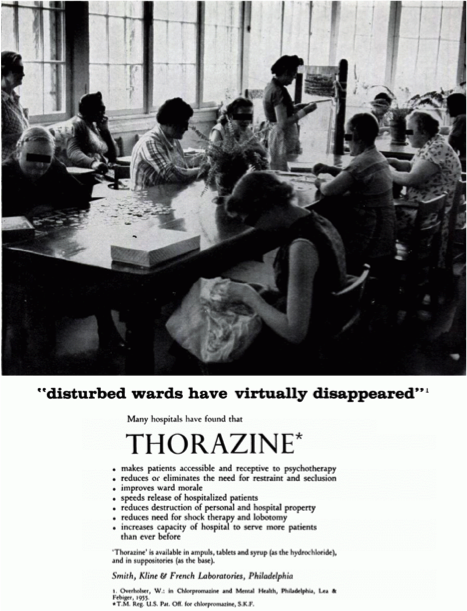
It was initially used with general anaesthesia to sedate and prevent shock(Carpenter and Davis 2012, 1168) and when trialled on patient Jacques Lh. undergoing ECT, an improvement of psychiatric symptoms was observed (Ban 2007). This was replicated by Deniker and Delay, who announced in Luxemburg that Chlorpromazine reduced psychosis symptoms(Carpenter and Davis 2012). Following this, Chlorpromazine saw the wards of asylums grow calm as noisy schizophrenic patients became quieter and more docile (Elkes and Elkes, 1954, 560), thus reducing violence and the number of hospitalised patients. Hence, despite some side effects like tardive dyskinesia, it became regarded as a miracle drug (Ban 2007, Carpenter and Davis 2012)
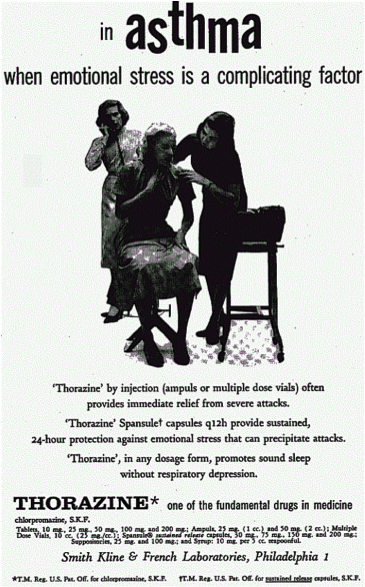
Following moral therapy’s failure, antipsychotics offered the possibility of a scientific and medical approach that shifted the location of clinical care(Carpenter and Davis 2012, 1168). It wasn’t long before advertisements began marketing Chlorpromazine at not only schizophrenia, but also emotional instability, hiccups and cancer (APA 1956, 2; APA 1958), highlighting the lack of understanding of the mechanisms of the drug. Over time the uses became more specific and psychopharmacology grew rapidly and chlorpromazine prompted the development of the dopamine hypothesis (Carpenter and Davis 2012, 1170).
5. 980- The Diagnostic and Statistical Manual of Mental Disorders-III
 Figure 6: DSM-III
Figure 6: DSM-III
The third edition (1980) of the APA’s DSM (Diagnostic and Statistical Manual of Mental Disorders), was revolutionary for the diagnosis and treatment of mental illness (Decker 2013, xvii).
The DSM-III influenced psychiatry’s shift from an aetiological and psychoanalytic focus, towards descriptive classification (Decker 2003, xvi). Neo-Kraepelinian in nature, (Tsou 2016), it emphasised symptoms and course and aimed to provide clear and valid definitions (APA 2017). This was influenced by the 5-axis system implemented by Spitzer, who advocated for biological ideas (Decker 2013, 315-317). The manual was larger than it’s predecessors and involved the caveats that the criteria were not completely discrete, and should only be used by psychiatrists (APA 1980), for whom it became convenient shorthand.
The DSM-IIIs flaws can be seen through attempts of subsequent editions to rectify mistakes, such as homosexuality’s removal in 1973 (Cooper 2004, 6) and some argue that it has not managed to progress beyond description (Tsou 2016). The criteria were not as clear or evidence based as intended, and symptom thresholds excluded many people from diagnosis (Cooper 2004, 5-22). Nevertheless, the DSM-III was a milestone document due to its descriptive diagnostic categories and the support for which it gave to the disease model (Decker 2013). It was the first DSM to become widely used by professionals and provide a uniform method of diagnosis (Tsou 2016).
The results of electrically induced seizures in a patient called Enrico X, were presented at the 3rd International Neurological Congress (1939), with a reported significant reduction of symptoms (Shorter and Healey 2007, 43), from which ECT rose to popularity in the 1940s. Early on, seizures would result in physical harm and this led to the development of muscle relaxants and use of anaesthetics (Piotrowski and Guerra 2016).
Despite initial popularity, in the 1980s antipsychiatry and politics resulted in rapid decline in the use and reputation of ECT, damage that is still being reversed today (Shorter and Healey 2007, 145). ECT’s development is significant as it is an empirical treatment that can produce rapid responses to acute symptoms of psychosis and depression (Shorter 1997, 3).